Prepared with the support of:

Child maltreatment (sexual abuse, physical abuse, neglect) results in a yearly economic burden of $124 billion1 Approximately 4 million reports are made to Child Protective Services (CPS) each year involving 7.4 million children [2]. Of these reports 3.5 million are investigated and 12.5% of children in the U.S. will be victims of substantiated maltreatment by age 18 [3]. Regardless of substantiation [4], CPS involvement is associated with a host of negative outcomes including subsequent maltreatment, teen motherhood, poor mental health, HIV, and substance use [5-6]. Almost 40% of children are re-referred to CPS following an initial referral [7-8] and 20% of victims of child maltreatment are re-victimized within 5 years.
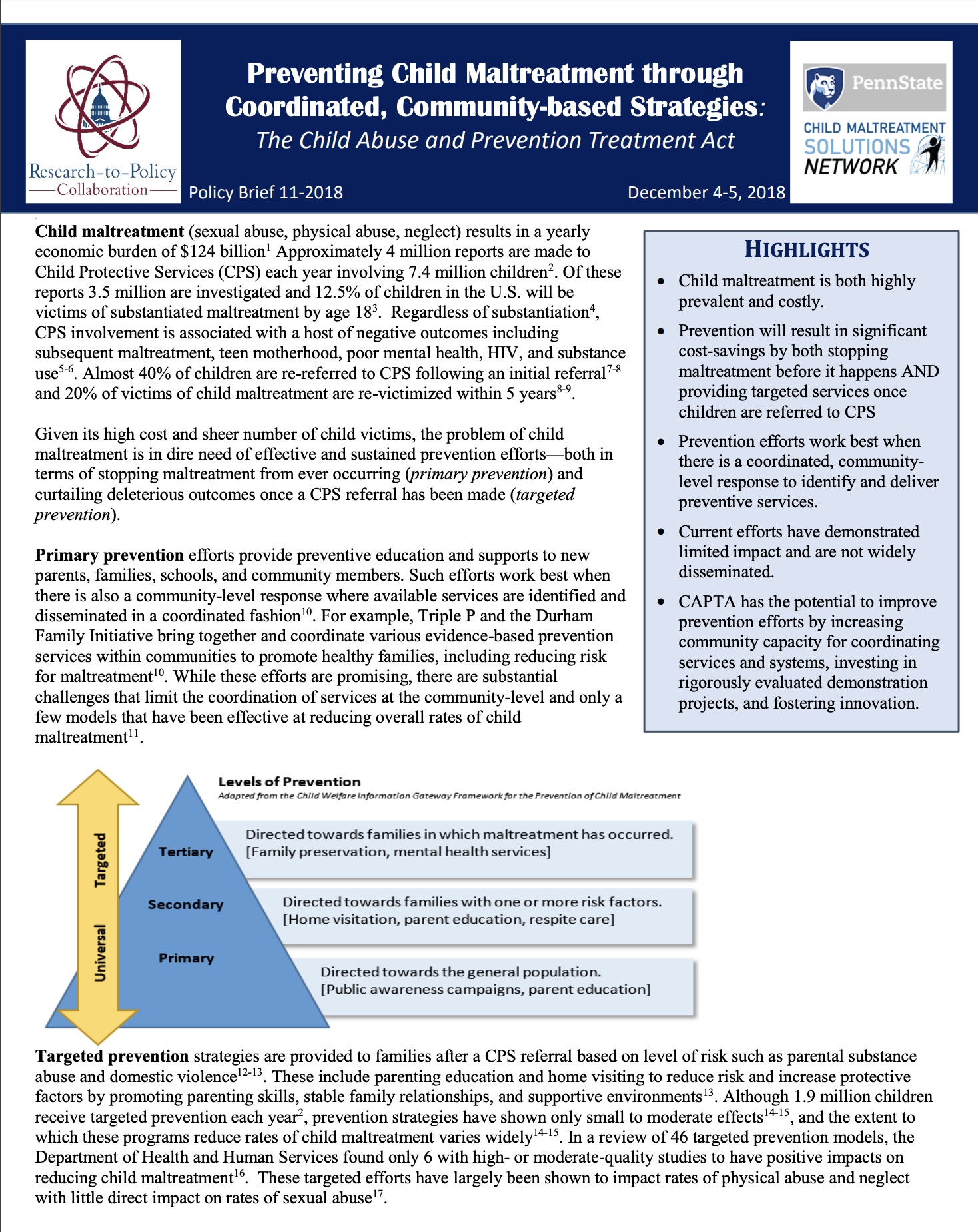
Given its high cost and sheer number of child victims, the problem of child maltreatment is in dire need of effective and sustained prevention efforts—both in terms of stopping maltreatment from ever occurring (primary prevention) and curtailing deleterious outcomes once a CPS referral has been made (targeted prevention).
Highlights
- Child maltreatment is both highly prevalent and costly.
- Prevention will result in significant cost-savings by both stopping maltreatment before it happens AND providing targeted services once children are referred to CPS
- Prevention efforts work best when there is a coordinated, community- level response to identify and deliver preventive services.
- Current efforts have demonstrated limited impact and are not widely disseminated.
- CAPTA has the potential to improve prevention efforts by increasing community capacity for coordinating services and systems, investing in rigorously evaluated demonstration projects, and fostering innovation.
Primary Prevention efforts provide preventive education and supports to new parents, families, schools, and community members. Such efforts work best when there is also a community-level response where available services are identified and disseminated in a coordinated fashion [10]. For example, Triple P and the Durham Family Initiative bring together and coordinate various evidence-based prevention services within communities to promote healthy families, including reducing risk for maltreatment [10]. While these efforts are promising, there are substantial challenges that limit the coordination of services at the community-level and only a few models that have been effective at reducing overall rates of child maltreatment [11].

Targeted prevention strategies are provided to families after a CPS referral based on level of risk such as parental substance abuse and domestic violence [12-13]. These include parenting education and home visiting to reduce risk and increase protective factors by promoting parenting skills, stable family relationships, and supportive environments [13]. Although 1.9 million children receive targeted prevention each year [2], prevention strategies have shown only small to moderate effects [14-15], and the extent to which these programs reduce rates of child maltreatment varies widely [14-15]. In a review of 56 targeted prevention models, the Department of Health and Human Services found only 6 with high- or moderate-quality studies to have positive impacts on reducing child maltreatment [16]. These targeted efforts have largely been shown to impact rates of physical abuse and neglect with little direct impact on rates of sexual abuse [17].
- Investments in prevention strategies are fragmented and minimal. Existing resources to prevent child maltreatment are distributed from disconnected sources (e.g., MIECHV, TANF, Title IV-E and –B, and CAPTA and CBCAP). States and communities must combine and leverage these funding streams in various ways to adequately serve child welfare families. The Community-Based Child Abuse Prevention (CBCAP) grants are currently the only funding sources dedicated exclusively to prevention, yet comprise only 0.45% of child welfare program funding [18].
- Current prevention efforts are underdeveloped and inadequately researched [19].
Prevention strategies must be improved to maximize impact. The rates of re-referrals and re-occurrences of substantiated maltreatment in the CPS system, paired with small to moderate effects of prevention programs, underscores the importance of prevention and intervention efforts. Programs funded by CBCAP vary in terms of being evidence-based, have limited resources for evaluation, and have not been evaluated over all [19-20]. There is a need for increased evaluation capacity [20] at the community-level in order to better understand which strategies are effective. Further, additional research is necessary to better understand how to integrate services and resources in a cost-effective manner. CAPTA funds can be used for demonstration projects, but an overall evaluation of the effectiveness has not been conducted. Further, few changes made to CAPTA by past reauthorizations have ever been evaluated for effectiveness20. Thus, research and evaluation should be prioritized to address improvements and foster innovation within CAPTA and CBCAP, as well as the research and evaluation priorities set forth by Congress.
CAPTA has the potential to strengthen the impact of prevention efforts. The CAPTA reauthorization presents an opportunity to strengthen current prevention efforts by (1) increasing communities’ capacity for prevention service coordination and continuous quality improvement efforts, (2) investing in demonstrations of local innovations in prevention coupled with rigorous evaluation, and (3) addressing Congress’ research priorities.
End Notes / References
- Fang, X., Brown, D. S., Florence, C. S., & Mercy, J. A. (2012). The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect, 36, 156-165.
- U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2017). Child Maltreatment 2016. Available from https://www.acf.hhs.gov/sites/default/files/cb/cm2016.pdf.
- Wildeman, C., Emanuel, N., Leventhal, J. M., Putnam-Hornstein, E., Waldfogel, J., & Lee, H. (2014). The prevalence of confirmed maltreatment among US children, 2004 to 2011. JAMA Pediatrics, 168, 706-713.
- Kohl, P. L., Jonson-Reid, M., & Drake, B. (2009). Time to leave substantiation behind: Findings from a national probability study. Child Maltreatment, 14, 17-26.
- Kugler K. C., Guastaferro K., Shenk C. E., Beal S. J., Zadzora K. M., & Noll, J. G. (2018) The effect of substantiated and unsubstantiated investigations of child maltreatment and subsequent adolescent health. Child Abuse & Neglect, 1-8.
- Jonson-Reid M., Kohl P. L., & Drake B. (2012) Child and adult outcomes of chronic child maltreatment. Pediatrics, 5, 839-845.
- Kohl, P. L., Jonson-Reid, M., & Drake, B. (2009). Time to leave substantiation behind: Findings from a national probability study. Child Maltreatment, 14, 17-26.
- Connell, C. M., Bergeron, N., Katz, K. H., Saunders, L., & Tebes, J. K. (2007). Re-referral to child protective services: The influence of child, family, and case characteristics on risk status. Child Abuse & Neglect, 31, 573-588.
- Fluke, J.D., Shusterman, G.R., Hollinshead, D., & Yuan, Y.T. Rereporting and Recurrence of Child Maltreatment: Findings from NCANDS. (Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, 2005).
- Daro, D., & Dodge, K. A. (2009). Creating community responsibility for child protection: possibilities and challenges. The Future of Children, 19, 67-93.
- Prinz, R. J., Sanders, M. R., Shapiro, C. J., Whitaker, D. J., & Lutzker, J. R. (2009). Population-based prevention of child maltreatment: The US Triple P system population trial. Prevention Science, 10, 1-12.
- Brown, J., Cohen, P., Johnson, J. G., & Salzinger, S. (1998). A longitudinal analysis of risk factors for child maltreatment: Findings of a 17-year prospective study of officially recorded and self-reported child abuse and neglect. Child Abuse & Neglect, 11, 1065-1078.
- Centers for Disease Control and Prevention. Child abuse and neglect: Risk and protective factors. Available from: http://www.cdc.gov/ViolencePrevention/childmaltreatment/riskprotectivefactors.html
- Geeraert, L., Van den Noortgate, W., Grietens, H., & Onghena, P. (2004). The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: A meta-analysis. Child Maltreatment, 9, 277-291
- Chen M, Chan KL.(2016). Effects of parenting programs on child maltreatment prevention a meta-analysis. Trauma, Violence, Abuse, 17, 88-104.
- U.S. Department of Health and Human Services. Home visiting evidence of effectiveness.
- Mendelson, T., & Letourneau, E. J. (2015). Parent-focused prevention of child sexual abuse. Prevention Science, 16, 844-852.
- Congressional Research Services (2018). Child welfare: An overview of federal programs and their current funding. Available from: https://www.everycrsreport.com/files/20180102_R43458_9a7c2ce137b54096617803ba8c171c543c4575b0.pdf
- IOM (Institute of Medicine) and NRC (National Research Council) (2018). New directions in child abuse and neglect research. Washington, DC: The National Academies Press. Available from: https://www.ncbi.nlm.nih.gov/books/NBK195985/pdf/Bookshelf_NBK195985.pdf
- FRIENDS National Center for Community-Based Child Abuse Prevention. (2016). 2016 CBCAP report summary: Our collective impact. Available from: https://friendsnrc.org/files/98/2016-Digital-Summary/1821
The Research-to-Policy Collaboration (RPC) works to bring together research professionals and public officials to support evidence-based policy. Please visit their website to learn more.
Key Information
RPC Website
Research-to-Policy Collaboration
More RPC Resources
RPC Resources
Publication DateDecember 1, 2018
Topic Area(s)Social Services
Resource TypeWritten Briefs
Share This Page
Prepared with the support of:
Child maltreatment (sexual abuse, physical abuse, neglect) results in a yearly economic burden of $124 billion1 Approximately 4 million reports are made to Child Protective Services (CPS) each year involving 7.4 million children [2]. Of these reports 3.5 million are investigated and 12.5% of children in the U.S. will be victims of substantiated maltreatment by age 18 [3]. Regardless of substantiation [4], CPS involvement is associated with a host of negative outcomes including subsequent maltreatment, teen motherhood, poor mental health, HIV, and substance use [5-6]. Almost 40% of children are re-referred to CPS following an initial referral [7-8] and 20% of victims of child maltreatment are re-victimized within 5 years.
Given its high cost and sheer number of child victims, the problem of child maltreatment is in dire need of effective and sustained prevention efforts—both in terms of stopping maltreatment from ever occurring (primary prevention) and curtailing deleterious outcomes once a CPS referral has been made (targeted prevention).
Highlights
- Child maltreatment is both highly prevalent and costly.
- Prevention will result in significant cost-savings by both stopping maltreatment before it happens AND providing targeted services once children are referred to CPS
- Prevention efforts work best when there is a coordinated, community- level response to identify and deliver preventive services.
- Current efforts have demonstrated limited impact and are not widely disseminated.
- CAPTA has the potential to improve prevention efforts by increasing community capacity for coordinating services and systems, investing in rigorously evaluated demonstration projects, and fostering innovation.
Primary Prevention efforts provide preventive education and supports to new parents, families, schools, and community members. Such efforts work best when there is also a community-level response where available services are identified and disseminated in a coordinated fashion [10]. For example, Triple P and the Durham Family Initiative bring together and coordinate various evidence-based prevention services within communities to promote healthy families, including reducing risk for maltreatment [10]. While these efforts are promising, there are substantial challenges that limit the coordination of services at the community-level and only a few models that have been effective at reducing overall rates of child maltreatment [11].
Targeted prevention strategies are provided to families after a CPS referral based on level of risk such as parental substance abuse and domestic violence [12-13]. These include parenting education and home visiting to reduce risk and increase protective factors by promoting parenting skills, stable family relationships, and supportive environments [13]. Although 1.9 million children receive targeted prevention each year [2], prevention strategies have shown only small to moderate effects [14-15], and the extent to which these programs reduce rates of child maltreatment varies widely [14-15]. In a review of 56 targeted prevention models, the Department of Health and Human Services found only 6 with high- or moderate-quality studies to have positive impacts on reducing child maltreatment [16]. These targeted efforts have largely been shown to impact rates of physical abuse and neglect with little direct impact on rates of sexual abuse [17].
- Investments in prevention strategies are fragmented and minimal. Existing resources to prevent child maltreatment are distributed from disconnected sources (e.g., MIECHV, TANF, Title IV-E and –B, and CAPTA and CBCAP). States and communities must combine and leverage these funding streams in various ways to adequately serve child welfare families. The Community-Based Child Abuse Prevention (CBCAP) grants are currently the only funding sources dedicated exclusively to prevention, yet comprise only 0.45% of child welfare program funding [18].
- Current prevention efforts are underdeveloped and inadequately researched [19].
Prevention strategies must be improved to maximize impact. The rates of re-referrals and re-occurrences of substantiated maltreatment in the CPS system, paired with small to moderate effects of prevention programs, underscores the importance of prevention and intervention efforts. Programs funded by CBCAP vary in terms of being evidence-based, have limited resources for evaluation, and have not been evaluated over all [19-20]. There is a need for increased evaluation capacity [20] at the community-level in order to better understand which strategies are effective. Further, additional research is necessary to better understand how to integrate services and resources in a cost-effective manner. CAPTA funds can be used for demonstration projects, but an overall evaluation of the effectiveness has not been conducted. Further, few changes made to CAPTA by past reauthorizations have ever been evaluated for effectiveness20. Thus, research and evaluation should be prioritized to address improvements and foster innovation within CAPTA and CBCAP, as well as the research and evaluation priorities set forth by Congress.
CAPTA has the potential to strengthen the impact of prevention efforts. The CAPTA reauthorization presents an opportunity to strengthen current prevention efforts by (1) increasing communities’ capacity for prevention service coordination and continuous quality improvement efforts, (2) investing in demonstrations of local innovations in prevention coupled with rigorous evaluation, and (3) addressing Congress’ research priorities.
End Notes / References
- Fang, X., Brown, D. S., Florence, C. S., & Mercy, J. A. (2012). The economic burden of child maltreatment in the United States and implications for prevention. Child Abuse & Neglect, 36, 156-165.
- U.S. Department of Health & Human Services, Administration for Children and Families, Administration on Children, Youth and Families, Children’s Bureau. (2017). Child Maltreatment 2016. Available from https://www.acf.hhs.gov/sites/default/files/cb/cm2016.pdf.
- Wildeman, C., Emanuel, N., Leventhal, J. M., Putnam-Hornstein, E., Waldfogel, J., & Lee, H. (2014). The prevalence of confirmed maltreatment among US children, 2004 to 2011. JAMA Pediatrics, 168, 706-713.
- Kohl, P. L., Jonson-Reid, M., & Drake, B. (2009). Time to leave substantiation behind: Findings from a national probability study. Child Maltreatment, 14, 17-26.
- Kugler K. C., Guastaferro K., Shenk C. E., Beal S. J., Zadzora K. M., & Noll, J. G. (2018) The effect of substantiated and unsubstantiated investigations of child maltreatment and subsequent adolescent health. Child Abuse & Neglect, 1-8.
- Jonson-Reid M., Kohl P. L., & Drake B. (2012) Child and adult outcomes of chronic child maltreatment. Pediatrics, 5, 839-845.
- Kohl, P. L., Jonson-Reid, M., & Drake, B. (2009). Time to leave substantiation behind: Findings from a national probability study. Child Maltreatment, 14, 17-26.
- Connell, C. M., Bergeron, N., Katz, K. H., Saunders, L., & Tebes, J. K. (2007). Re-referral to child protective services: The influence of child, family, and case characteristics on risk status. Child Abuse & Neglect, 31, 573-588.
- Fluke, J.D., Shusterman, G.R., Hollinshead, D., & Yuan, Y.T. Rereporting and Recurrence of Child Maltreatment: Findings from NCANDS. (Washington, DC: U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation, 2005).
- Daro, D., & Dodge, K. A. (2009). Creating community responsibility for child protection: possibilities and challenges. The Future of Children, 19, 67-93.
- Prinz, R. J., Sanders, M. R., Shapiro, C. J., Whitaker, D. J., & Lutzker, J. R. (2009). Population-based prevention of child maltreatment: The US Triple P system population trial. Prevention Science, 10, 1-12.
- Brown, J., Cohen, P., Johnson, J. G., & Salzinger, S. (1998). A longitudinal analysis of risk factors for child maltreatment: Findings of a 17-year prospective study of officially recorded and self-reported child abuse and neglect. Child Abuse & Neglect, 11, 1065-1078.
- Centers for Disease Control and Prevention. Child abuse and neglect: Risk and protective factors. Available from: http://www.cdc.gov/ViolencePrevention/childmaltreatment/riskprotectivefactors.html
- Geeraert, L., Van den Noortgate, W., Grietens, H., & Onghena, P. (2004). The effects of early prevention programs for families with young children at risk for physical child abuse and neglect: A meta-analysis. Child Maltreatment, 9, 277-291
- Chen M, Chan KL.(2016). Effects of parenting programs on child maltreatment prevention a meta-analysis. Trauma, Violence, Abuse, 17, 88-104.
- U.S. Department of Health and Human Services. Home visiting evidence of effectiveness.
- Mendelson, T., & Letourneau, E. J. (2015). Parent-focused prevention of child sexual abuse. Prevention Science, 16, 844-852.
- Congressional Research Services (2018). Child welfare: An overview of federal programs and their current funding. Available from: https://www.everycrsreport.com/files/20180102_R43458_9a7c2ce137b54096617803ba8c171c543c4575b0.pdf
- IOM (Institute of Medicine) and NRC (National Research Council) (2018). New directions in child abuse and neglect research. Washington, DC: The National Academies Press. Available from: https://www.ncbi.nlm.nih.gov/books/NBK195985/pdf/Bookshelf_NBK195985.pdf
- FRIENDS National Center for Community-Based Child Abuse Prevention. (2016). 2016 CBCAP report summary: Our collective impact. Available from: https://friendsnrc.org/files/98/2016-Digital-Summary/1821
The Research-to-Policy Collaboration (RPC) works to bring together research professionals and public officials to support evidence-based policy. Please visit their website to learn more.
Key Information
RPC Website
Research-to-Policy Collaboration
More RPC Resources
RPC Resources
Publication DateDecember 1, 2018
Topic Area(s)Social Services
Resource TypeWritten Briefs
Share This Page
LET’S STAY IN TOUCH
Join the Evidence-to-Impact Mailing List
Keep up to date with the latest resources, events, and news from the EIC.